
Sandrena Gel and Weight Loss – What’s Really Going on?
When you come across Sandrena Gel, you’re looking at a hormone replacement therapy (HRT) product, not a magic slimming gel. Its main purpose is to restore oestrogen levels in menopausal women. Yet, some discussions suggest it may influence weight – for better or worse. Honestly, the truth is more nuanced and less glamorous than some might hope.
What Is Sandrena Gel?
Sandrena Gel contains the active ingredient Estradiol (a form of oestrogen) and is a transdermal HRT product. It is prescribed for the relief of menopausal symptoms such as hot flushes, night sweats, vaginal dryness and mood shifts.
Key facts:
- It’s applied to clean, dry skin (typically thighs or lower abdomen) and allowed to absorb.
- It’s worth noting that Sandrena Gel isn’t designed for weight management or slimming. Still, some women have mentioned that after starting the treatment, their weight shifts slightly downwards. That may happen because restoring hormone balance can sometimes help regulate appetite and metabolism – but the change is usually minimal and not the main effect of the therapy.
- Dosage generally starts at 0.5 mg and may go up to 1.5 mg daily.
Does Sandrena Gel Lead to Weight Loss?
Let’s be clear: the evidence that Sandrena Gel produces weight loss is weak. According to the official product information, weight gain is listed among common side-effects.
But notes that users may lose a little weight when using Sandrena Gel because restoring hormone balance can help regulate metabolism and appetite – but significant weight loss would not be expected.
Sandrena Gel is not designed for weight change, but for menopausal symptoms.
My interpretation
So – yes, weight loss could occur, but only modestly and indirectly. Here are reasons why it’s unlikely to be dramatic:
- Weight is influenced by many factors: diet, exercise, genetics, hormone levels, age, sleep, stress. A gel cannot override all of that.
- HRT via transdermal oestrogen like Sandrena may improve metabolism or muscle-mass preservation in menopause. But “improve” does not mean “slim you down rapidly”.
- Some women may experience fluid retention or bloating initially with HRT, which can mask weight loss.
In short: if you hope to use Sandrena Gel as a weight-loss tool, you’ll likely be disappointed. Its role is menopausal relief – any weight effect is secondary.
Considerations and Risks
If you are considering Sandrena Gel (for menopausal symptoms) and are curious about weight impact, bear in mind:
- Expectation management: Approach the therapy for what it’s approved for. Expecting weight loss may lead to frustration.
- Lifestyle still matters: Balanced diet, regular exercise, good sleep and stress management remain the core of weight control. The gel may help some of the hormonal background, but cannot replace lifestyle.
- Monitor side-effects. Sandrena Gel carries risks: weight gain, fluid retention, headaches, breast tenderness.
- Discuss with your doctor: Your prescribing clinician can guide dosage, monitor your hormone levels and advise on risks vs benefits.
Practical Advice: If You’re Using Sandrena Gel and Want to Optimise Weight-Related Benefits.
If you are already prescribed Sandrena Gel or considering it, and weight is a concern, you might speak with your doctor about the dose and any relevant lifestyle modifications.
It’s generally recommended to keep a simple log of your diet, physical activity, and how you feel over the months. Try to focus on resistance or muscle-strengthening exercises, as these can help support your metabolism. Stay well hydrated and pay attention to any signs of fluid retention – if you notice unusual swelling, it’s best to mention it to your doctor.
Be patient – hormone therapies often take weeks to truly settle (some sources say a few days to weeks for effect; full benefits may take up to three months).

My Verdict
If I were to summarise candidly: Sandrena Gel is a solid tool for menopausal symptoms, but a poor one for weight loss. If you think you’ll apply the gel and watch the kilos fall away, you will likely be disappointed. It might help with underlying hormone shifts that make weight control harder in menopause – and in that sense it’s indirectly helpful – but it won’t do the heavy lifting for you.
In a way, it’s like putting the engine in a car – you still need to steer, fuel it, brake sensibly, and pick the right road. The engine (Sandrena) helps, but the journey (lifestyle, diet, exercise) is yours.
So: yes, you can possibly expect a slight improvement in how your body handles weight because your hormonal environment is more stable. But no – don’t expect dramatic weight drop or treat the gel as a weight-loss prescription.
The Bottom Line
In summary, you may consider Sandrena Gel if you’re experiencing symptoms of menopause and your doctor recommends it. But if your primary motivation is weight loss, think twice – and talk frankly with your doctor. The therapy might help you regain some metabolic control, but it should not be seen as a shortcut or substitute for good habits.
Be realistic, be patient, and integrate it into a broader plan of healthy living. If weight loss is a goal, pair the HRT with sound nutrition, movement and proper support. Anything else would be an unfair promise – and in my view, misleading.
Sean Rigby Weight Loss – What We Know, What We Don’t, and What Matters
Why This Became a Story
Fans of “Endeavour” noticed a slimmer Jim Strange when series eight arrived in September 2021. Lifestyle sites and TV blogs picked it up. The talk was simple – Sean Rigby looked leaner on screen. No scandal. No speech. Just a visible change that viewers clocked straight away.

Rigby plays Jim Strange, Morse’s steady foil, across “Endeavour” from its early years to the 2023 finale.
The Facts Versus the Noise
Here’s the honest bit. There’s no on-record interview where Rigby details how or why he lost weight. Much that circulates online is guesswork or recycled fan chatter. Treat any claimed numbers with caution – sources that throw out exact stones or pounds tend to be blogs repeating each other. My view: if the actor hasn’t said it, we shouldn’t pretend he did. The only solid claim is the on-screen change noticed by reviewers and viewers in 2021.
What We Can Say with Confidence
“Endeavour” wrapped in 2023. Promotional stills and recaps show Rigby as Strange through that final run, looking markedly trimmer than in early seasons. That confirms the change wasn’t a one-episode blip. It held.
My Take – and Yes, It’s a Bit Blunt
Speculation sells. But bodies are not press releases. The fair position is simple – applaud the work, and let the person keep what they want private. If you still want a lesson, it’s this: steady change shows up on camera, even if no one narrates it.
What Viewers Noticed
A quick scan of coverage from the week series eight launched shows two themes. First, people were surprised – “almost unrecognisable” was the vibe in reviews and tweets. Second, the chatter quickly slid back to plot. That tells you something. Novelty fades; performance stays. Possibly that’s the best compliment.
What to Ignore
You’ll find posts shouting about secret detoxes, miracle overnight drops. Hard pass. The credible route is dull on purpose – marginal gains layered for months. The NHS advice backs that up: plan meals, track portions, move most days, keep going.
Keep Actor and Character Separate
Jim Strange’s weight is not a plot point. The series doesn’t turn his size into a story arc, so any change you noticed is off-screen life, not a scripted twist. It’s easy to blur the lines – possibly because we watch these characters for years – but it’s worth keeping lanes clear.
Practical Moves You Can Actually Stick to
- Plan tomorrow tonight – write down meals and one activity slot. Removing guesswork beats willpower. The NHS plan encourages this week-by-week structure.
- Walk more by default – add steps to commutes and errands; if formal workouts feel heavy, light daily movement still counts toward the targets.
- Protect muscle – two strength sessions a week help metabolism and long-term maintenance; body-weight work is fine.
- Track one metric – food, steps, or minutes moved. Consistency beats complexity.

Red Flags Worth Dodging
- Crash diets – dramatic restriction boomerangs. The 12-week approach is designed to be gradual and repeatable.
- Miracle claims with a celebrity face – if a site uses a star’s name to sell an exact “secret method” without sources, close the tab.
- Exercise “hacks” – there isn’t one. The evidence line is clear: 150 minutes moderate or 75 vigorous each week, plus strength work. Do the basics well.
How to Follow a Celebrity Weight Story
Curiosity is fine – prying isn’t. When you read about a body-change story, start with what has a spine. Look for on-record quotes, proper interviews, and coverage from credible outlets. Pay attention to change that shows up more than once – not a single angle or a single week. And prefer a health-first frame over gossip: food quality, movement, sleep, stress. Skip the fluff. Overnight transformations don’t match biology.
If a story nudges you to act, translate it into something you can repeat. Pick two daily anchors – protein with veg, and a short walk you’ll keep even on bad days. Add simple strength work twice a week when you’re ready. Treat sleep as a pillar, not a perk. Measure inputs you control – meals cooked at home, steps taken, sessions done – rather than obsessing over the scale.
Why the “How Much Did He Lose?” Question Misses the Point
Numbers can motivate, but they also trap you. If you chase a headline figure, you risk swings you can’t live with. Better to pick measures you control – meals cooked at home, steps, sleep. That’s dull. It’s also how change survives a bad week.
The Bottom Line
Sean Rigby’s leaner look in “Endeavour” is real on screen. The method remains his business. The lesson for the rest of us isn’t a hack – it’s momentum. Eat closer to whole foods. Move most days. Use strength work twice a week. Possibly you’ll feel different in a fortnight. Keep going and you might look different in a season or two. The camera – and your clothes – will notice.
Tim Montgomerie Weight Loss – What’s Real and What’s Useful
Why People Are Asking
Searches for “Tim Montgomerie weight loss” keep popping up. Fair enough – public figures talk about health and it sparks curiosity. Here’s the honest bit: there’s no verified, on-record account from Tim setting out kilos lost, exact diet rules, or a gym plan. What does exist is his public commentary on weight loss, willpower, and modern tools like weight-loss jabs. That’s the ground we can stand on – and use.

What He’s Said in Public
On TV and YouTube debates, Tim has been blunt. In one clip he frames unhealthy eating as, at least partly, a willpower issue. That’s unpopular in some circles – but he said it anyway. In another panel he floats a pragmatic line on weight-loss medicines: if a safe “wonder drug” works, why not use it. You may disagree. You may nod. Either way, these quotes show his stance on personal choice and modern aids.
What We Don’t Know – and Shouldn’t Pretend to
There’s no credible source giving his personal before-after numbers, nor a step-by-step “Tim diet”. If you see a precise figure attached to his name, treat it as speculation unless it’s directly from him or a reputable outlet quoting him. I won’t dress it up – the internet loves a number. Accuracy loves restraint.
The Useful Middle Ground
You don’t need a celebrity blueprint to get moving. The boring truths still work. The NHS is clear: weight change comes from managing energy in vs energy out – and doing it in a way you can keep up. Counting every morsel isn’t mandatory, but understanding calories helps. Pair that with activity guidelines and you’re no longer guessing.
Two Things That Actually Shift the Dial
Food you can repeat:
- Aim for protein and plants at most meals – fish, eggs or pulses plus veg.
- Swap refined starches for whole grains – oats, whole-wheat, brown rice.
- Keep ultra-processed snacks for rare moments – not daily habits.
- Use olive oil, but measure it – “healthy” still has calories.
- Drink water or tea. Save sugary drinks for treats.
Activity you’ll do when you’re tired:
- The UK guidance: about 150 minutes a week of moderate work – brisk walking, cycling – plus two sessions for strength.
- Spread it out. Ten to twenty minute chunks still count.
- If joints complain, try swimming or a bike.
- When you’re ready, add hills, intervals, or longer walks.

Where Weight-Loss Medicines Fit
Tim’s on-air line was practical – if a safe medicine helps, consider it. The NHS position is careful: medicines can play a role, but they sit on top of diet, movement, and behaviour change. Not instead. If you’re curious, your GP can explain options and eligibility. Don’t buy mystery vials online – you know how that ends.
Sleep, Stress, and the Stuff We Ignore
Sleep isn’t soft. Poor sleep drives appetite and nudges you toward quick sugar and fat. Fix the basics: regular bedtime, darker room, less late scrolling. Stress pushes in the same direction. A short walk, a call to a friend, or even five minutes of breathing can stop a raid on the biscuit tin. It sounds small – it’s not.
Is weight loss only willpower?
No. Biology fights back. Food environments are noisy. But willpower still matters on the margin – at the point of decision. You build it by shrinking the number of hard choices you face each day: plan meals, keep defaults simple, remove easy junk from the house. Then you need less willpower, not more. That’s the boring secret. Tim’s provocation pushes that point, even if the tone ruffles feathers.
A One-Week Frame You Can Actually Keep
- Breakfast – oats with yoghurt and berries; or eggs with tomatoes and spinach.
- Lunch – chickpea salad with peppers and olive oil; or tuna on whole-wheat toast.
- Dinner – salmon with broccoli and brown rice; or chicken and veg stir-fry.
- Snacks – fruit, nuts, plain yoghurt; water or tea.
- Activity – five brisk 30-minute walks; two short strength sessions at home.
It’s not glamorous. It works.
What to Do If You’re Stuck
Two moves: tighten portions by 100–200 kcal per day – or add a 15-minute walk after meals. If nothing shifts after six to eight weeks, get help – a GP, a registered dietitian, or the NHS Digital Weight Management Programme. Honest help beats heroic isolation.
Bottom Line
“Tim Montgomerie weight loss” isn’t a dossier – it’s a doorway into a bigger conversation. He’s argued for personal agency and, yes, for using medical tools where they’re appropriate. You don’t need his numbers to act. Build a repeatable plate. Walk more. Lift something. Sleep enough. Possibly try clinical support if you qualify. Do the small things daily – and keep the noise low. That’s the part that lasts.
Vidya Balan Weight Loss – Diet First, Noise Later
Why This Story Landed Now
Vidya Balan has been open about her body for years. Then came a leaner look and a frank admission: the change came from food, not the gym. She said her long fight with weight was misread – much of it was “inflammation”, not fat – and that a Chennai nutrition team helped her reset. The internet did the rest.
What She Actually Said

In late 2024 interviews, Vidya explained she met a group called Amura in Chennai. Their view: calm the inflammation first. She cut foods that didn’t suit her, followed an elimination-style plan, and – her words – didn’t work out that year. She credits the shift to that process, not punishing training or crash diets. Honestly, that’s rare in celebrity talk.
In those on-record clips and mainstream write-ups she did not state kilograms or pounds herself. Coverage focused on the method and the “inflammation, not fat” idea, plus the temporary pause on exercise. Some outlets later put a figure on it. One widely shared piece claimed she lost “around 10 kg” with the diet and zero exercise. Treat that as a media estimate – not a direct quote – because she hasn’t confirmed a precise total publicly. Honestly, that matters. If a number isn’t from the person herself or from a clinical context, you hold it lightly.
The Inflammation Angle – No Magic, Just Pattern
“Anti-inflammatory diet” sounds mystical. It isn’t. Mainstream guides boil it down to whole foods, plenty of plants, olive oil, nuts, and fatty fish. Fewer ultra-processed hits. Fewer added sugars. Think Mediterranean-leaning plates rather than detox rituals. Possibly dull on paper – effective in practice.
What to Put on the Plate
Let’s keep it practical. Here’s a clear, credible list you can use today.
Foods to embrace:
- Vegetables – broccoli, kale, peppers, Brussels sprouts, cabbage, cauliflower.
- Deep-coloured fruit – blueberries, cherries, grapes, pomegranate, citrus.
- Healthy fats – olive oil, avocado, olives.
- Fatty fish – salmon, sardines, mackerel, herring, anchovies.
- Nuts, seeds, spices – almonds, walnuts, turmeric, cinnamon.
What to dial down:
- Ultra-processed snacks and sweets – fast calories, little upside.
- Refined grains in bulk – white breads, pastries.
- Deep-fried foods and processed meats – more palatable energy than you think.

Did She Really Stop Working Out?
She said so – “first year I haven’t worked out”. I don’t recommend that as a general rule. Exercise protects mood, muscle, and long-term health. But her team tested food triggers first and paused training while doing it. Her case, her context. If you’re tempted to copy-paste, talk to a professional.
How This Fits with Evidence
Anti-inflammatory eating patterns are well described. They focus on antioxidants, fibre, omega-3 fats, and fewer refined products. That can lower inflammatory markers and often makes a calorie deficit easier without counting every bite. You feel steadier. You snack less. Weight may follow. It’s not a miracle – it’s a nudge built into everyday food.
My Read on the “Inflammation, Not Fat” Line
The line is provocative. Strictly, inflammation isn’t body fat. But inflammation can drive water retention, appetite signals, and fatigue that push weight up. When you remove certain foods and improve diet quality, bloat falls and energy rises. That’s a visible shift. Possibly that’s most of the early change. The rest is consistency.
What You Can Borrow – Without the Hype
This isn’t a celebrity blueprint. It’s a set of levers you can pull.
Six simple levers:
- Veg at two meals – half the plate if you can.
- Protein each meal – fish, eggs, pulses, yoghurt.
- Olive oil as your default fat – measure it; “healthy” still has calories.
- Whole grains over refined – oats, brown rice, whole-wheat.
- Spices on everything – turmeric, pepper, herbs.
- Sleep 7–8 hours – appetite hormones care about sleep.
Two guardrails:
- Don’t ditch training long-term unless a clinician tells you to – movement is non-negotiable for health.
- If you suspect intolerances, test with a registered dietitian; DIY elimination can spiral into needless restriction.
Honest Limits
A transformation story isn’t a clinical trial. “Anti-inflammatory” isn’t a single, regulated protocol. Results vary. If your overall intake still overshoots your needs, you won’t lose weight on olives and salmon either. I’m not here to scold – just to keep the physics in view. Food quality helps you keep a small, steady deficit. That’s the point.
A One-Week Frame You Can Actually Follow
- Breakfast – oats with blueberries and walnuts; or eggs with tomatoes and spinach.
- Lunch – chickpea and pepper salad with olive oil and lemon; or grilled sardines on whole-wheat toast.
- Dinner – salmon with broccoli and brown rice; or dal with cabbage stir-fry.
- Snacks – fruit, plain yoghurt, a small handful of nuts; tea or water.
It’s simple, repeatable, and – crucially – not joyless.
Bottom Line
Vidya Balan’s shift put food at the centre and framed weight through the lens of inflammation. I like the honesty. I also think we should keep our feet on the ground. Eat closer to how your grandparents cooked, cut the ultra-processed noise, use olive oil, and keep protein steady. Possibly you’ll feel lighter in a fortnight. Keep going for months and the scale may follow. The internet loves a before-after. Real life loves a routine.
Inositol and Weight Loss – What the Evidence Really Says
What Is Inositol?
Inositol is a sugar-like compound your body makes and you also get from foods such as beans, grains and fruit. Supplements usually use two forms – myoinositol (MI) and D-chiroinositol (DCI). They act inside cells as messengers for hormones, including insulin. That’s the simple story, and it matters for weight because insulin signalling touches appetite, glucose control and fat storage.
How Could It Help With Weight?
The pitch is straightforward: improve insulin sensitivity, steady blood sugar, curb hunger a little. There’s clinical support in insulin-resistant settings. For example, a randomised trial in gestational diabetes found myoinositol (4 g/day) improved insulin resistance and raised adiponectin – a hormone tied to better metabolic health. Possibly that’s one reason some people notice easier appetite control.
What Does the Research Say About Weight Loss?
Here’s the uncomfortable truth – effects on body weight are real but modest.
- A 2022 meta-analysis of 15 trials reported a small reduction in BMI with inositol versus control (weighted mean difference – 0.41 kg/m²). Useful, but not dramatic.
- In polycystic ovary syndrome (PCOS), evidence is stronger: a 2023 meta-analysis of 26 RCTs showed BMI fell more with inositol than placebo (mean difference – 0.45 kg/m²). Myo-inositol specifically showed a slightly larger drop (- 0.71 kg/m²). Benefits also appeared in glucose markers and androgens. Still, we’re talking centimetres, not clothing sizes.
If you’re expecting results like GLP-1 medicines, you’ll be disappointed. If you’re aiming for a nudge in the right direction, especially with PCOS or insulin resistance – this fits.
Who Might Benefit Most?
People with features of insulin resistance often do best in studies – PCOS, gestational diabetes, sometimes metabolic syndrome. Outside those groups, data are thinner and the size of effect shrinks. I’m not saying “don’t try it”. I’m saying set expectations low and build the basics around it.
Dosing and Forms
Most trials used myoinositol at 2 g twice daily (total 4 g/day). Some combine MI and DCI in a 40:1 ratio; evidence still leans toward plain MI for metabolic outcomes. High-dose MI (around 12 g/day) can cause gut upset – not worth it for weight. If you’re going to test it, start with the studied doses, give it 8–12 weeks, then judge.
Foods to Boost Your Intake
You don’t have to live on powders or pills. Inositol shows up in everyday food, and, honestly, that’s the easiest win. Classic food surveys found the richest sources in fruits, beans, grains and nuts, with fresh produce tending to edge out canned or frozen. Your body also makes some inositol on its own, but diet can still nudge things in the right direction.
Good food sources to keep in rotation:
- Fruits – oranges, grapefruit, melon (especially cantaloupe).
- Legumes and pulses – beans and peas in all their forms.
- Whole grains – oats, whole-wheat breads, brown rice, bran-heavy cereals.
- Nuts and seeds – almonds, walnuts; peanut butter counts too.
- Other everyday sources – corn and a range of meats also contribute smaller amounts.
Simple ways to use them
- Stir citrus segments or diced cantaloupe through yoghurt, quick breakfast, no drama.
- Build a bean and whole-grain rice salad – olive oil, lemon, herbs.
- Go for oats or high-bran cereal, then add almonds or walnuts on top.
- Swap to whole-wheat toast with peanut butter when you need a fast snack.
A quick caution that keeps things honest: a lot of plant inositol is stored as phytic acid in grains and legumes. Our gut microbes can release some of it, but the yield varies. Soaking, sprouting or fermenting may change how much is available, yet the net effect isn’t identical for every food. In short: eat these foods plus your supplement.

Safety and Side Effects
Inositol is generally well tolerated. The most common issues are nausea, bloating or diarrhoea, usually at higher doses and typically mild. If you take medications that affect glucose, speak to your clinician first – you don’t want unexpected dips. Pregnancy and long-term use deserve medical advice as standard.
How to Use It Well
Do this:
- Pair it with a protein-rich, high-fibre diet and regular movement – resistance work plus brisk walking is a solid base.
- Be consistent with dosing – mornings and evenings.
- Track something – waist, clothes fit, or a simple habit streak.
Avoid this:
- Dosing creep “just in case”. Your gut will complain.
- Sugary toppings to “reward” your supplement. That defeats the point.
- Using it instead of evidence-based treatment when you have diabetes or severe insulin resistance.
The PCOS Angle
PCOS is where inositol earns its keep. Trials show improvements in ovulatory cycles, androgens and metabolic markers, with side-effect rates often lower than metformin. Weight changes are small, yet the cluster of benefits adds up. If you have PCOS and struggle with standard options, inositol is a reasonable adjunct to discuss.
My Take
If you’re already dialling in sleep, protein, steps, and stress – inositol may give you that last 5% nudge. If the basics are chaos, it won’t rescue you. Honestly, I like it as an adjunct for people with PCOS or clear insulin-resistant traits. For everyone else, I’d label it “maybe” – affordable, low-risk, but not a fat-loss accelerator. You might feel steadier appetite. You might not. Test, measure, decide.
Practical Starting Plan
- Confirm your goal and timeline – slow loss is fine.
- Talk to your GP or pharmacist if you take glucose-affecting meds.
- Trial myoinositol 2 g twice daily for 12 weeks.
- Keep protein ~1.2–1.6 g/kg/day, fibre 25–35 g/day, steps 7–10k.
- Reassess: if weight or waist hasn’t budged at all, park it.

Bottom Line
Inositol is not a silver bullet for weight loss. It is a small lever that seems to help most in insulin-resistant states – with the best evidence in PCOS, and it’s generally safe at studied doses. Use it as part of a bigger plan, not instead of one.
Is Weetabix Good for Weight Loss? Brief Look
What Weetabix Brings to the Table
When the morning alarm goes off and you reach for breakfast, what you choose can set the tone for your whole day. Weetabix is often pitched as a solid start – two biscuits deliver around 136 kcal, about 3.8 g fibre, 1.6–1.7 g sugars and low fat. It has wholegrain wheat, iron, B-vitamins and a “green traffic light” label for fat, sugar and salt. Fine so far.
So: does that make it an effective weight-loss breakfast? Possibly – but only if you play the rest of your day well.
Why It Could Help with Losing Weight
There are a few reasons one might pick Weetabix as part of a weight-loss plan:
| Fibre content | At 3.8 g fibre per serving it helps slow digestion and may support fuller feelings after breakfast. |
| Low sugar and low fat (for a cereal) | Many breakfast options are stacked with sugar or hidden fat. Here the numbers are modest. |
| Simple portion size and clarity | Two biscuits is easy. 136 kcal gives you a baseline. In short, it can anchor your breakfast in a lower-calorie, higher-fibre zone. For people chasing a calorie-deficit, that is useful. |
Why It Isn’t a Magic
Let’s get honest, this isn’t a “lose 10 kg in two weeks” solution. There are caveats. 136 kcal is fine – but if you add full-fat milk, honey, syrup, lots of fruit and nuts, your breakfast may end up 250-300 kcal or more. The cut advantage fades. The fibre is okay – but 3.8 g is not huge. For weight-loss you benefit from higher fibre and also moderate-to-higher protein. Weetabix is modest on protein. Breakfast is one meal. If lunch, snacks and dinner are heavy you’ll undo the head start. Managing weight requires more than one good meal. Buyers point out that the carbohydrate load (26 g carbs per serving) still raises blood sugar and may leave you somewhat hungry later.
So yes: Weetabix can help – but only as part of a broader plan.
How to Use It Smartly for Weight Loss
Here are some practical tweaks to make this cereal work better:
Smart Practices
- Stick to two biscuits + semi-skimmed or skimmed milk (or alternative); aim for < 200 kcal for breakfast.
- Add fresh fruit (berries, banana) for fibre and nutrients.
- Avoid adding lots of syrup, sugar or heavy toppings. That erases benefits.
Things to Watch
- If you’re active and need more calories, adjust – maybe add yoghurt or seeds, but still mind total intake.
- Monitor afternoon hunger – if you’re starving by 11.30, the breakfast might not be enough for you.
- Remember that owning a breakfast cereal doesn’t give licence for overeating later.

What the Research and Experts Say
According to Diabetes UK, Weetabix scores well – two biscuits provide 136 kcal, 26 g carbs and just 1.7 g sugar. The cereal also appears in journalist listings of “better breakfast cereals” based on fibre, sugar and processing.
However, no large long-term weight-loss trial uses Weetabix as the intervention. It’s a good food, not a weight-loss therapy. The weight-loss effect depends on what you do around it: total calories, movement, sleep, stress.
Straight Talk
Let’s keep it blunt. If you swap a high-sugar, high-fat breakfast for two biscuits of Weetabix + milk + berries, you are likely to eat fewer calories and get more fibre. That shift alone can help you lose weight. But if you think “I’ll eat Weetabix and relax the rest of my diet” – you’ll be disappointed.
Weight loss is like painting a room: you need the primer, the colour, the finishing touches. Weetabix can be the primer – but you still need the other coats. Use it wisely.
Who It Works Well for – and Who May Need More
Good fit:
- Someone who eats big breakfasts, wants to cut calories without feeling deprived.
- Someone who needs a convenient, consistent breakfast they can build on.
Might not be enough on its own: - If your lunch and dinner are uncontrolled, breakfast won’t counterbalance it.
- If you need higher protein in the morning (e.g., you train heavily, build muscle), you might prefer a higher-protein breakfast.
- If you snack frequently mid-morning due to unstable blood sugar, you may need a breakfast with more sustaining elements than cereals alone.
Final Thoughts
Yes – Weetabix can be a part of a weight-loss strategy. It hits many of the right notes: low sugar, wholegrain, simple portion. But no – it is not a standalone weight-loss solution. If you want sustainable results you must work the rest of the day too. Activity, good sleep, hydration, boundaries on snacks… these things still matter. Possibly you’ll lose more weight by focusing on your lunch and dinner than obsessing over cereal. Let’s keep it realistic. Breakfast cereals like Weetabix help – but they don’t replace the rest of the picture. As stated on its official website, “The key to a healthy diet is balance. No one food provides all the nutrients (food components) you need for health.”
Amycretin Weight Loss Pill – Promise, Proof and Practical Reality
Why Amycretin Has Everyone Talking
Obesity remains a global health challenge – millions seek effective solutions. Enter Amycretin, a new drug from Novo Nordisk that aims for more than incremental gains. It combines two mechanisms in one molecule – GLP-1 receptor agonism and amylin receptor agonism. That sounds impressive. But the truth is more nuanced. Possibly it heralds a breakthrough. Honestly, we need to ask tough questions.
What Amycretin Actually Is
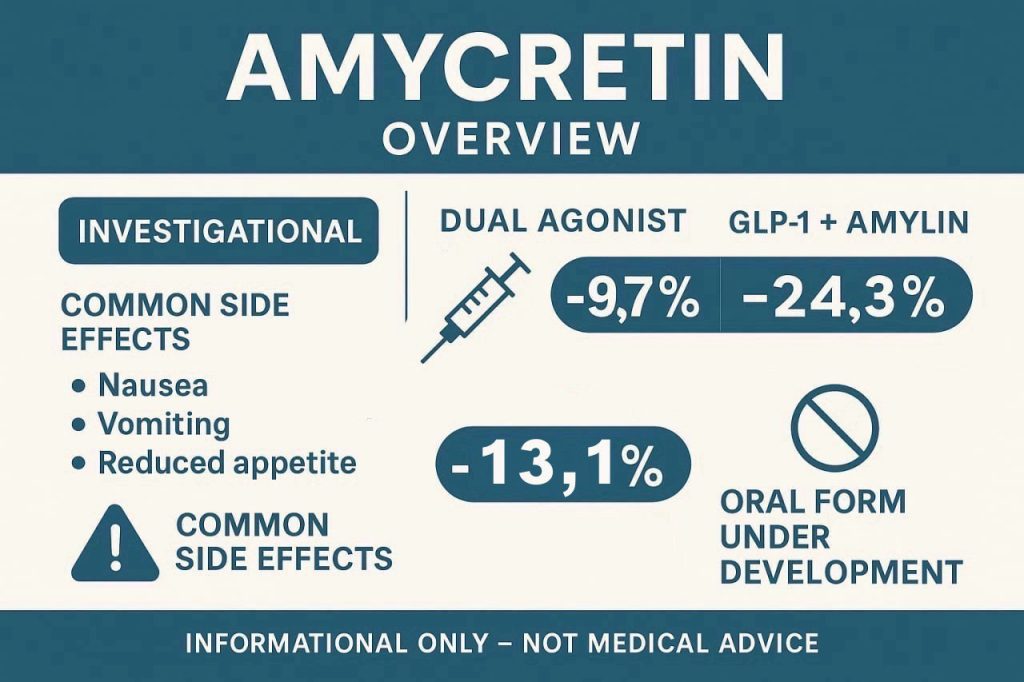
Amycretin is a long-acting, unimolecular drug designed for people with overweight or obesity (and potentially type 2 diabetes later). Unlike drugs that focus only on GLP-1, Amycretin also targets the amylin pathway. GLP-1 helps insulin secretion and slows gastric emptying. Amylin complements that by promoting satiety and further slowing digestion. By hitting both, the theory is you get stronger weight-loss effects.
Clinical Trial Results – the Numbers
Here are the key findings from early trials. In the Phase 1b/2a subcutaneous trial with 125 participants doses of:
- 1.25 mg for 20 weeks led to ~ 9.7% weight loss;
- 5 mg for 28 weeks led to ~ 16.2%;
- 20 mg for 36 weeks led to ~ 22%
In contrast, placebo groups had weight gains of ~1.9-2.3%. At the highest dose (60 mg) in one cohort, weight loss reached ~24.3% at week 36. In a daily oral formulation (Phase 1) participants lost up to – 10.4% (the maximum dose – 13.1%) body weight after 12 weeks.
These results suggest Amycretin may outperform existing medications – but they are early, small scale, and subject to many caveats.
What the Trials Show and Don’t
What trials show is promising: bold weight-loss numbers, dual-mechanism innovation, safety profile consistent with known drug classes.
What they don’t show yet: real-world durability, long-term safety, comparisons with established treatments, full regulatory approval. The drug remains investigational and not available in the UK.
Side Effects & Safety
Common side effects mirror other GLP-1/amylin therapies: nausea, vomiting, reduced appetite, gastrointestinal upset. Most events were mild or moderate. Rarely discussed publicly yet: long-term effects, rare adverse events, how the drug will behave in people with multiple comorbidities or on other medicines. In short – safety is good so far, but not settled.
Practical Considerations
If you’re watching this drug because you live with obesity or overweight, here’s where things stand for you:
- Availability: Not licensed yet in the UK. You cannot get Amycretin through prescription now.
- Cost: Unknown. New drugs often cost a lot – access may be limited.
- Lifestyle remains vital: Drugs help, but they don’t replace basic habits.
- Timing: Phase 3 trials planned early 2026. Approval and clinical adoption may take years.
My Honest Opinion
I’ll be blunt – I think Amycretin represents real hope. The weight-loss percentages are significant and suggest the dual mechanism could matter. But I also think we must temper expectations. The hype often runs ahead of evidence. People may expect instant “miracle pill” results – that is risky. Until long-term data land, and until traditional measures – diet, physical activity, behaviour – are still part of the story, you’re betting on something promising but still in the lab.
Who Might Benefit – and Who Should Wait
May benefit:
- Someone with obesity and risk factors who is willing to wait for new treatments and to engage fully in lifestyle change.
- Someone who has tried current therapies without success and is following research developments.
Should wait:
- If you need treatment now and cannot wait for approval or coverage.
- If you prefer established treatments with known access and support.
- If you believe a pill or injection alone will fix everything – that mindset sets you up to be disappointed.
Summary Takeaways
- Amycretin is a dual-agonist approach targeting GLP-1 and amylin.
- Early trials show up to ~ 22-24% weight loss in 36 weeks; oral form shows ~13% in short term.
- Safety profile so far acceptable, but long-term data missing.
- Not yet approved in the UK; real-world applicability unknown.
- It’s promising – but not a finished solution. Your lifestyle still counts more than ever.

Final Verdict
Yes – Amycretin may be a game-changer. Possibly it will shift the benchmark for weight-loss drugs. But let’s not get ahead of the data. If you are looking for solutions today, don’t let potential future drugs distract you from what works now: consistent eating habits, movement you can sustain, sleep, behaviours. Amycretin might one day join the tools; today, it’s a serious candidate under investigation. If you ask me – wait for approval, ask your clinician, stay realistic. That’s the honest truth.
Trim Patch & Weight Loss – Hype, Hope, or Hard Pass?
What a “Trim Patch” Actually Is
A trim patch is a small adhesive square you stick on your skin. It sits in the same family as nicotine or HRT patches – the transdermal route. Makers say the patch releases “actives” that bypass the gut and reach the bloodstream. The promises are familiar: fewer cravings, faster metabolism, weight loss while you sleep. Honestly – that’s a tidy story with little hard proof behind it. Clinical guidance says there’s no robust evidence that over-the-counter slimming patches cause meaningful, sustained weight loss.
The Evidence – What We Know and What We Don’t
Let’s separate marketing from data. Medical sites reviewing the field are blunt: there are no good human trials showing that generic weight loss patches work. None that are peer-reviewed, randomised, and adequately powered. That’s the minimum for confidence.
How Transdermal Delivery Works – and Where It Struggles
Transdermal drug delivery is real medicine. Nicotine, oestrogen, and pain medicines use it well. But getting sizeable, plant-based molecules through the skin barrier is hard. Recent reviews describe the workarounds – enhancers, microemulsions, microneedles – and still emphasise the limits, the variability, and the need for better standards. That’s a long way from a cosmetic patch that claims to burn fat.
Do Weight-Loss Patches Work?
Short answer – not on the evidence we have. Consumer health sources that survey the literature highlight a lack of peer-reviewed, adequately powered human trials for slimming patches. Without randomised trials and measured outcomes, you cannot claim reliable weight loss.
What Regulators and Watchdogs Say
When patches have promised dramatic loss, regulators have stepped in. The US Federal Trade Commission has banned sellers and fined marketers for unsubstantiated “diet patch” claims – and keeps warning the public about red-flag weight-loss ads. That history matters; it tells you how shaky these claims have been.
The US Food and Drug Administration also flags a wider problem: weight-loss products sold online are often contaminated or mislabelled, and some vendors now trade on “GLP-1” buzz with unapproved formulations. The agency urges people to avoid unapproved or misbranded products sold direct to consumers. If a site hints at GLP-1-like effects in a patch, be sceptial.
What Trim Patch Reviews Say
You asked about public sentiment. As of today, the Trustpilot page shows a low “Bad” TrustScore with fewer than a few dozen reviews. Read the comments yourself; they are mixed to negative and raise issues about results. Reviews are not clinical data – but they are a temperature check. Also remember: review ecosystems can be noisy and sometimes gamed. Treat any star rating as one input, not the final word.
What Actually Works Long-Term
Let’s keep it practical. Sustainable weight change comes from a stack of small levers – not a single gadget. NHS-style basics endure because they work across many people and contexts.
Focus on the fundamentals
- A regular eating pattern with enough protein, fibre, and minimally processed foods.
- Calorie awareness without obsession – gentle deficit, measured over weeks.
- Movement most days – brisk walking, resistance work, something you don’t hate.

Layer in Support Where Appropriate
- Behavioural tools for stress, sleep, and emotional eating.
- Discuss approved medications if BMI and risk justify them – GLP-1s, for example, are prescription-only and backed by trials.
- Health checks for thyroid, medications that drive weight, or other conditions.
Why Patches Keep Selling Anyway
Patches promise three things: no pills, no injections, no effort. They also use science-like language – “thermogenesis”, “bioavailability”, “hormone support”. The fine print rarely shows dose delivered to blood, changes in appetite hormones, or weight outcomes in humans. You get anecdotes and before-after photos instead of trials. The internet loves a tidy miracle; biology does not.
Where “Trim Patches” Might Fit – If at All
If you use a patch as a reminder – a daily nudge to choose a walk over a snack – fine. Just don’t outsource the work to an adhesive square. The likely effect, based on current evidence, is small to none. If a product claims “lose weight while you sleep” or “GLP-1 benefits without a prescription”, be sceptical. Honestly – save your money for decent food and good shoes.
Bottom Line
Trim patches offer a neat story – stick, forget, slim. The science doesn’t back it. If you choose to experiment, do so with eyes open and expectations low. Better yet, spend your effort where the return is proven – a workable food plan, movement you can repeat, and, if appropriate, licensed treatments discussed with a professional. That’s not a catchy slogan. It’s how people actually keep weight off.
Marcus Mumford’s Weight Loss – What Actually Changed
Why This Story Landed Now
Marcus Mumford turned up in summer 2025 looking leaner – and the internet did what it does. The spark was a run of posts from New Orleans, where Lainey Wilson guested with Mumford & Sons and shared backstage shots. Fans noticed the transformation first, then headlines followed. The attention wasn’t just vanity. It tied to something he’d already said out loud: he’d lost about 70 pounds.
What He Said About The Weight
In March 2025, comedian Caleb Pressley asked the question straight: “You lost 70 pounds?” Mumford didn’t duck it. “Yeah… I had to stop eating ice cream.” It was a throwaway line, delivered with a grin, but it told you the gist – fewer nightly treats, more structure. Honesty plays well. So does brevity.
When The Shift Began
This didn’t happen overnight. Back in 2022, on Radio X, Mumford explained that training gave him a fresh sense of purpose beyond music and family. He talked about a new “reward system” – more centred on surfing than ice cream. That’s a tidy frame: swap the dopamine source, keep the joy. Possibly that’s the whole game.
What We Can Infer – Carefully
He has not published a plan. No macro counts. No before-after grid. But you can map the themes from his own words and appearances:
- Reduce energy-dense “rewards” – in his case, ice cream.
- Add consistent movement – he name-checked surfing.
- Make it stick – two-plus years tell you this wasn’t a crash.
That’s not a celebrity secret. It’s behaviour change. Boring, effective, repeatable.
The Public Moment In New Orleans
The “near-unrecognisable” headlines ramped up after Wilson’s Instagram posts from the New Orleans show in early August 2025. People Magazine and other outlets covered the duet and the backstage content. You saw a trimmer frontman; you also saw a musician having fun. Both matter – weight loss without life is a bad trade.

Why Fans Care
Fans project. We see a frontman get lighter and wonder if we could. Here’s the blunt part – results vary. Genetics, schedules, stress, and food environments all push back. But Mumford’s framing helps. He didn’t sell a miracle. He swapped a nightly comfort for a daily practice. Honestly, that’s the only kind of story that lasts.
What His Life Context Adds
Context explains staying power. Mumford and his wife, actor Carey Mulligan, have three children. Their backstory is well known now – childhood pen pals, letters, even faxes, then a reconnection as adults. That kind of durable bond can make lifestyle changes easier to defend when touring and press tempt you back into old patterns. Possibly it’s a quiet advantage.

What This Doesn’t Prove
Let’s be clear about limits:
- We don’t know his exact diet or training volume.
- We don’t have medical markers, only images and quotes.
- We can’t assign credit to one behaviour.
Drawing hard lines from soft data is a common internet mistake. Don’t do it here. The safer conclusion is modest: habits changed; body followed.
If You’re Looking For Takeaways
No celebrity plan will fit you perfectly. Still, you can steal the scaffolding:
- Pick a “reward” you can live with – walking, swimming, surfing, anything that feels like play.
- Remove or reduce the nightly sugar bomb. Not forever, just most nights.
- Build a two-year horizon, not a two-week sprint.
That’s it. Simple doesn’t mean easy. But simple survives travel days, family life, studio sessions – and your equivalent of all three.
With The Edges Left On
Transformation stories often read like sermons. This one lands closer to a field note. He looks different. He says the work started years ago. He swapped treats for movement. That’s not sexy. It works. If you want a slogan: change the reward, keep the joy. If you want a warning: the internet loves an “unrecognisable” photo, then forgets the years it took to get there. Your timeline is yours. Don’t chase someone else’s montage.
Sources You Can Check
- Radio X 2022 conversation on fitness focus and the “reward system” shift to surfing. (Radio X)
- New Orleans collaboration posts and coverage showing the leaner appearance and timeline. (People.com)
- Public recounting of the pen-pal backstory on Good Morning Britain and follow-up write-ups. (AOL)
Orforglipron: the Weight-Loss Pill to Watch – What We Know Now
If you’ve been waiting for a pill instead of a weekly shot, orforglipron may be the candidate on your radar. It’s an oral GLP-1 receptor agonist – a class known for appetite and weight effects – taken once a day. The idea is simple: keep the biology of GLP-1, lose the needles. Reality is messier, as always, but the evidence is building.
What is orforglipron, in plain terms?
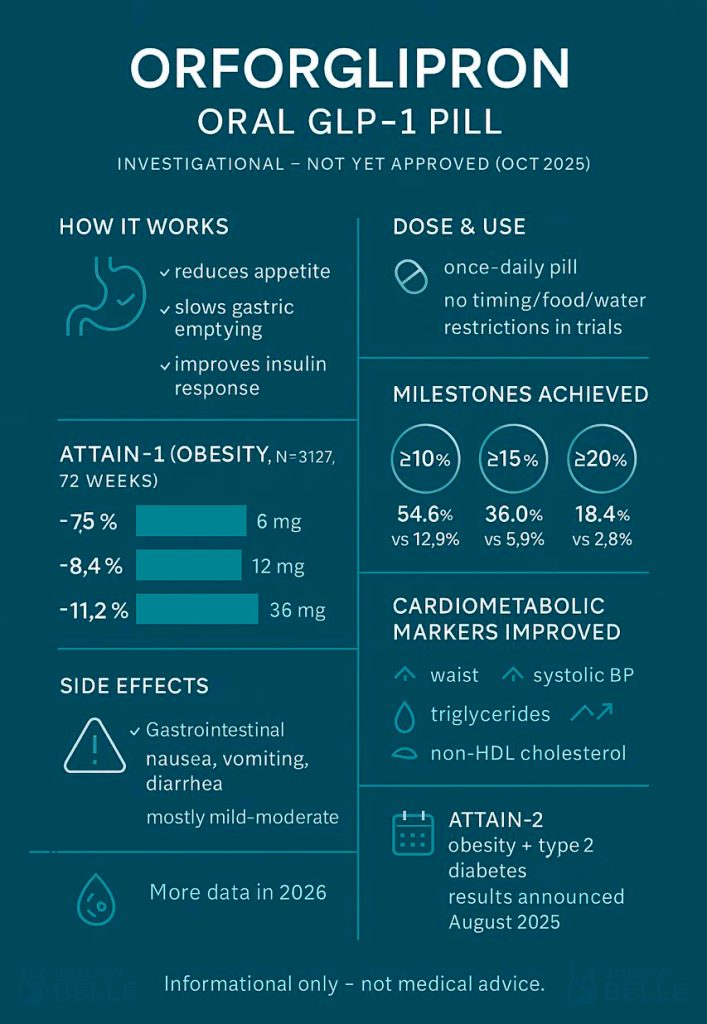
It’s a small-molecule, non-peptide GLP-1 receptor agonist designed for type 2 diabetes and for obesity treatment. Unlike peptide GLP-1s you inject, this comes as a tablet. In trials it was dosed once daily – without specific timing, food, or water restrictions – which, honestly, is the draw for many of you who dislike injections or complex dosing rules. It’s still investigational; no approvals yet anywhere.
How much weight loss are we talking about?
ATTAIN-1, a 72-week Phase 3 trial in adults with obesity but without diabetes (n≈3,100), reported average weight reductions of roughly 7.5% with 6 mg, 8.4% with 12 mg, and 11.2% with 36 mg, versus ~2.1% for placebo. More people on the highest dose hit the bigger milestones too: ≥10%, ≥15%, and ≥20% body-weight loss were all notably more common than with placebo. If you’re doing the mental math, a 10% drop is often the clinical “line in the sand” for risk reduction – and many participants crossed it.
Cardiometabolic picture – not just the scale
Beyond weight, markers moved in the right direction: waist circumference, systolic blood pressure, triglycerides, and non-HDL cholesterol improved more with orforglipron than with placebo. Possibly that’s the bigger story long-term, because risk is what we’re trying to bend. Still, results vary, and your baseline risk matters.
Safety and tolerability – the part everyone skims (please don’t)
The most common side effects were gastrointestinal – think nausea, vomiting, diarrhea – usually mild to moderate. Discontinuations due to adverse events happened in roughly 5–10% on orforglipron versus ~3% on placebo. If you’ve followed GLP-1s, that profile will look familiar. It’s not a free lunch – and if your gut is sensitive, you’ll want a candid conversation with your clinician.
Where things stand with regulators
As of mid-October 2025, orforglipron is not approved. Lilly says it plans to file for obesity in 2025 and for type 2 diabetes in 2026, with availability depending on how reviews go. There’s industry chatter about the FDA’s new fast-track voucher program, but the company has been cautious in public – so don’t bank on shortcuts. Possibly fast, possibly not. Patience helps.
How it stacks up against other treatments
Two diabetes-focused Phase 3 readouts this October matter for the broader story. In one trial, orforglipron cut A1C by up to ~1.7% and outperformed dapagliflozin (an SGLT2 inhibitor). In another, adding orforglipron to insulin glargine drove A1C down even further. Weight also moved in the right direction. That’s diabetes data, not an obesity head-to-head, but it suggests metabolic potency consistent with the class. A separate head-to-head against oral semaglutide in type 2 diabetes was also positive for orforglipron. The pill looks competitive – with the usual caveats about different populations and endpoints.
What we know so far
- Orforglipron is a once-daily oral GLP-1 RA, studied for obesity and type 2 diabetes; not approved yet.
- In ATTAIN-1 (72 weeks), mean weight loss ranged about 7.5%–11.2% across doses vs ~2.1% with placebo, with meaningful cardiometabolic gains.
- GI effects are common; discontinuations were ~5–10% on drug vs ~3% on placebo.
- Regulatory filings for obesity are planned for 2025; diabetes filings expected in 2026.
What we don’t know (yet)
- Real-world adherence when the novelty fades – pills can be “easier,” but daily routines fail.
- How it compares directly with leading injectables for obesity over 1–2 years – we need head-to-head obesity trials, not just diabetes readouts.
- Long-term safety beyond the current dataset – larger, longer studies and post-approval surveillance will tell us more.
Who might consider it if approved
- You want GLP-1-like effects but prefer a pill over injections.
- You’ve had access or supply issues with injectables and need another route.
- You have obesity-related risks where a 10% weight loss could change your risk profile – and you’re prepared for GI trade-offs.
Who might pass (or wait)
- You’ve had tough GI reactions to GLP-1s and aren’t ready to try again.
- You’re chasing 15–20% weight loss and already respond well to injectables – you might want to see more head-to-head obesity data first.
- You need coverage now – and can’t sit through regulatory timelines.
Our take
If you’re looking for magic, you’ll be disappointed. If you’re looking for options, this is real progress. A daily pill that delivers steady, double-digit weight loss for a good chunk of users is not a small thing. It lowers friction – no pens, no needles – and that can mean persistence. Possibly that’s the quiet superpower here. But – and here comes the sharp edge – tolerability still matters, expectations still matter, and behavior still matters. A pill won’t rewrite physics. It can tilt the odds.

Practical notes if you’re planning ahead
Should orforglipron get the green light, talk to your clinician about dose, titration, and how to navigate GI effects. Plan for the basics: protein intake, fiber, fluids, and a movement routine you can stand. Keep labs on schedule. If side effects bite, don’t ghost your care team – adjust. Honestly, that’s where people win or lose with GLP-1s.
Bottom line
Orforglipron is a serious, once-daily oral contender in the GLP-1 era. The weight-loss and cardiometabolic data are credible; the convenience is obvious; the safety looks class-consistent. Approval isn’t guaranteed, but the trajectory is clear. If you want a needle-free path with proven biology, keep this on your shortlist – eyes open, expectations steady.